Sexuality
Dr. C. George Boeree
Ah, sex. Freud, and many others, felt that sex was the most significant motivator in human life. It's interesting that you die without food in a few weeks, without water in a few days, and without air in a few minutes. You will not die without sex (although you may want to). And yet, in the biological scheme of things, it is reproduction, not individual survival, that counts. Animals, including us humans, are supplied with powerful instincts that urge them on to having sex, sometimes at the cost of their own lives!
The science of sex only dates back about a century. The first major figure is Richard von Krafft-Ebing, who studied sexual "deviations" in the late 1800's. He popularized the term homosexuality, and fought to decriminalize it. On the negative side, he was convinced that women who have strong sexual appetites are quite abnormal.
Another early figure is Henry Havelock Ellis, who looked into the social aspects of sexuality in the late 1800's and early 1900's. He is a hero to both the homosexual community and the feminist movement. He insisted that homosexuality was both inborn and irreversible, a notion some people still don't accept. And he had the audacity to suggest that women have the similar sexual needs and desires as men! Margaret Sanger - famous for her efforts at promoting birth control at that time - referred to him as an "Olympian!"
Beginning in the 1930's, a Harvard entomologist name Alfred Kinsey started to systematically collect data on sexual practices. He found, for example, that 90% of the men he interviewed had masturbated, that 85% had engaged in premarital intercourse, and that 60% had engaged in oral sex. This of course shocked a conservative American public, who had (like their Victorian predecessors) been in heavy denial about this sort of thing!
His statistics on homosexuality were even more shocking: He found that 37% of men had had at least one homosexual interaction resulting in orgasm, that 10% of men had been exclusively homosexual for the last three years, and that 4% of men had been exclusively homosexual their entire lives. The general direction of these statistics has been supported again and again since then.
The Sexual Response Cycle
It was the famous team of Virginia Masters and William Johnson who, in the 1960's and 70's, gave us the details about the mechanics of sex. They observed and measured many thousands of volunteers and prostitutes engaging in intercourse, masturbation, and what not. Among the results of their work is the famous "sexual response cycle:"
Excitement involves the contraction of the muscles of the pelvis, the erection of the penis, and the lubrication of the vagina. There is, of course, also a less obvious >erection of the clitoris and lubrication of the penis.
The plateau phase is less a bit less clear and some researchers just consider it a part of excitement. In women, the outer third of the vagina begins to close about 30%, which seems to be natures way of making sure that the penis (and its produce) stays where it is as long as possible.
Orgasm is much more obvious. It is really just a matter of repeated reflexive contractions of a variety of muscles. In men, it includes ejaculation. Women take on the average 15 minutes to reach orgasm, which means that men typically orgasm first unless they pay special attention to their partners during foreplay.
Resolution is simply a matter of getting back to normal. There is also something known as a refractory period, which is the length of time it takes before the person is ready for another round of sex. In young men, it can be a matter of minutes. In most men, it is hours, even days. It has been argued that women do not have a refractory period, but that is likely a myth. On the other hand, it seems that some women can have several orgasms in close succession, called multiple orgasms. Most women, however, find that continued intercourse after one orgasm eventually becomes uncomfortable.
There used to be the idea that there were two kinds of orgasms women could have - clitoral or vaginal. Clitoral orgasms are achieved by contact with the clitoris. Vaginal orgasms, achieved by full intercourse, were considered better, more "mature." However, since Masters and Johnson, most sexologists believe that all orgasms are essentially clitoral. It should be noted that, even though the clitoris is the "epicenter" of orgasm, pretty much all of the pelvic floor, including the vagina, is pretty sensitive to stimulation.
Another rich source of myths is penis
size. Various studies have suggested that somewhere between 5 and
6 inches when fully erect is the usual range. The longest
medically verified penis was 13 1/2 inches long. But human beings
can't hold a candle (so to speak) to the African elephant, who can
sport an erection as long as 5 or 6 feet, or whales, with erections as
long as 9 or 10 feet and one foot in diameter! If male readers
are feeling a bit inferior, do not despair: The smallest human
penis on medical record is less than an inch long, fully erect.
At least you're not him.

Actual fountain in the Netherlands
The Non-Deviant "Deviations"
Many psychologists of the late 1800's and early 1900's believed that masturbation resulted in all sorts of physical and mental ills and should be stopped at any cost. Today the consensus is clear: Masturbation has no ill effects of any sort for men or women, girls or boys. What used to be referred to as "self-abuse" now goes by the delightful phrase "pleasuring oneself"! Only if it becomes compulsive does it become an issue of concern.
Of course, masturbation isn't really a deviation at all: Roughly 60% of men and 40% of women report having masturbated in the past year. Of men from 18 to 39, 28% do so more than once a week, 37% less than once a week, and 35% not at all. It seems that 5% of men and 11% of women report never having masturbated. On the other hand, 53% of men and 25% of women began masturbating by the time they were between 11 and 13 years old. Clearly, there is nothing wrong with not masturbating, either. (Janus, S., and Janus, C. The Janus Report on Sexual Behavior. 1993. New York: John Wiley & Sons. Laumann, E., Gagnon, J.H., Michael, R.T., and Michaels, S. The Social Organization of Sexuality: Sexual Practices in the United States. 1994. Chicago: University of Chicago Press.)
Oral sex is also considered a normal and healthy sexual practice. Oral sex performed on a man is called fellatio; performed on a woman, it's called cunnilingus. 3/4 of men and 2/3 of women acknowledge that they rather enjoy oral sex. 10% of men and 18% of women even report preferring oral sex to achieve orgasm over intercourse (Janus & Janus, 1993). On the other hand, not liking oral sex is perfectly normal and healthy as well.
Anal sex is far less accepted, and for
good reasons: It is painful for many women, and tends to be associated
with a desire
on the part of some heterosexual men to dominate women. 10% of men and
9%
of women say they have had anal sex in the past year (Laumann, Gagnon,
Michael,
Michaels, 1994). On the other hand, it is estimated that 50% of male
homosexuals
engage in anal sex as an approximation to vaginal sex.
Homosexuality is not considered
pathological today. It appears that there is and always has been
a proportion of the human population that is sexually attracted to
same-sex partners, and that this is more an inborn variation than a
matter of choice. There is a separate chapter on sexual
orientation here.
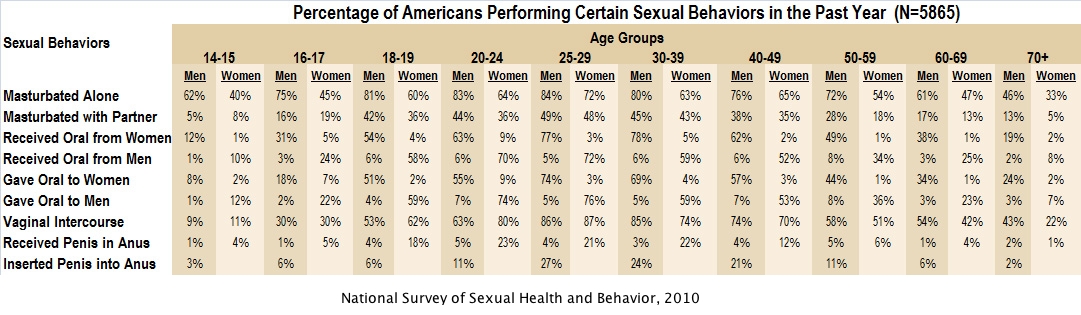
Here is a more recent survey on sexual
practices:
Sex and Adolescents
Although the ability to achieve orgasm is a neurological process present at birth, actual reproduction only occurs after the hormonal preparations provided by puberty. And so, while many grade-school boys and girls are interested in the opposite sex and may even be engaging in childhood versions of sexual activity (masturbation or "playing doctor", for example), it is in adolescence that sexuality becomes a real issue.
The average age of first intercourse in the US is 16.6 for boys and 17.2 for girls. Here is a more detailed account (NCHS, 1995):
Age at First Intercourse
Males FemalesAccording to another study from the Center for Disease Control and Prevention:
27% by age 15 25% by age 15
45% by age 16 39% by age 16
59% by age 17 52% by age 17
69% by age 18 65% by age 18
85% by age 19 77% by age 19
Among western, industrialized nations, only Russia and Estonia (both of which are suffering badly from the social turmoil resulting from the breakdown of the Soviet Union) have more teenage pregnancies and more teenage abortions than the United States. About one million teenagers -- 10% of girls between 15 and 19 -- become pregnant every year in the US! If you take out the girls who are virgins, 19% of all girls who have had intercourse get pregnant. (Teenage pregnancy: overall trends and state-by-state information. 1999. Alan Guttmacher Institute. New York: AGI.)
Most people who study these issues agree that, in addition to a sex-laden media, it is our conservative attitudes towards sex education that are primarily to blame: The US is one of the few countries in the world that routinely attempts to promote abstinence while assiduously avoiding making reference to other ways to avoid pregnancy and disease. One of our recent Surgeon Generals was forced to resign for the unpardonable sin of suggesting that we might make it clear to high school students that masturbation is a safe alternative to intercourse!
Not long ago, President Clinton was censured by the congress of the US for lying under oath about his relationship with a White House intern. He claimed that when he said he had not had sexual relations with her, he was only telling the truth: He did not consider oral sex to be sexual relations. Most people were astounded at the naiveté of that defense.
Unfortunately, it has come to light that a sizable proportion of southern college freshmen and sophomores (among others) think the same thing! 37% believed that oral sex is in fact sexual abstinence! In addition, 24% felt the same way about anal sex, and fully 61% felt that way about mutual masturbation.
(Horan PF, Phillips J and Hagan NE, The meaning of abstinence for college students, Journal of HIV/AIDS Prevention & Education for Adolescents & Children, 1998, 2(2):51-66. Reported in Remez, Lisa. Oral Sex Among Adolescents: Is It Sex or Is It Abstinence? Family Planning Perspectives Volume 32, Number 6, November/December 2000, available at http://www.agi-usa.org/pubs/journals/3229800.html#50a.)
In Los Angeles high schools, it was found that about 30% of virgins engaged in mutual masturbation, 10% of virgins engaged in oral sex, and 1% engaged in anal sex. Apparently, you can have sex and still be a virgin!
(Schuster MA, Bell RM and Kanouse DE, The sexual practices of adolescent virgins: Genital sexual activities of high school students who have never had vaginal intercourse, American Journal of Public Health, 1996, 86(11):1570-1576. Reported in Remez, 2000)
While sexual abstinence and monogamy are being taught to our teenagers, it seems that adults are having their own problems with the concepts. Here are some interesting statistics on adults:
Number of sexual partners since age 18
Men Women(Laumann, Gagnon, Michael, Michaels, 1994).
none 3% 3%
one 20 31
2 to 4 21 36
5 to 10 23 20
11 to 20 16 6
21 or more 17 3
It does get considerably better for married
people: About 80% of women and somewhere between 65 and 85% of
men say that they
had no sexual partners other than their spouse while married. 94%
of
married men and women say they only had sex with their spouse in the
last
year. But 5% had at least one partner other than their spouse --
with
1% saying they had over four other partners! (Laumann, Gagnon, Michael,
Michaels,
1994).
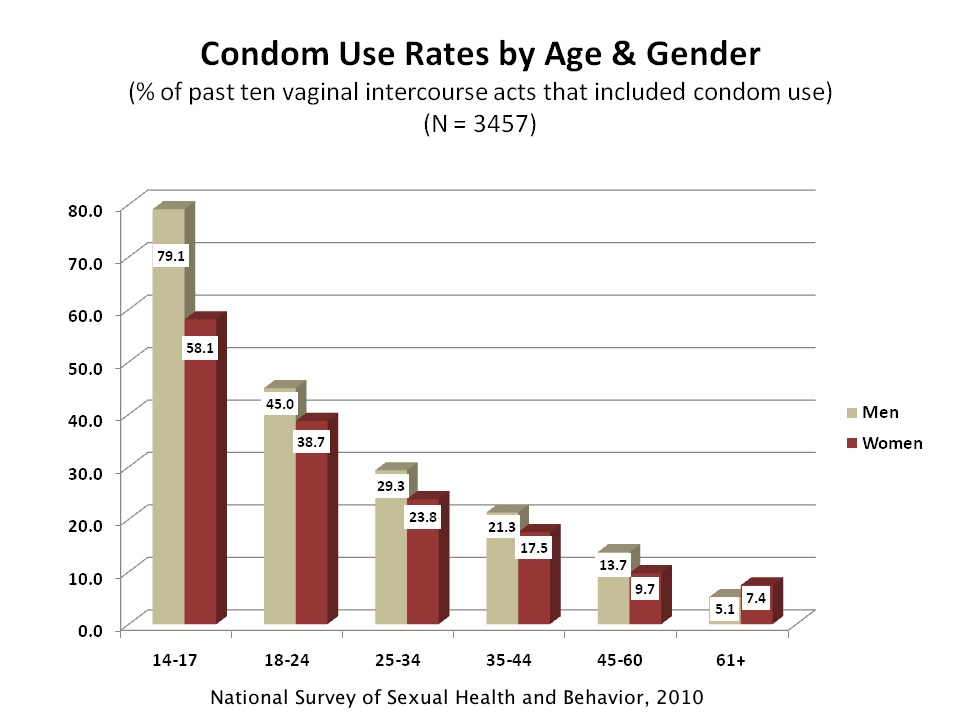
Here is a recent survey on condom use at
different ages. It could be
better:
Sexual Dysfunctions
With something as intense and pervasive as sex, you've got to expect that things go wrong. The standard categorization of sexual disorders comes out of the DSM IV, which is a manual designed by psychiatrists that describes mental illnesses and labels them for ease of communication and standardization of diagnoses.
First, there are the sexual dysfunctions, which involve problems with sexual desire or performance:
Hypoactive sexual desire disorder is a "deficiency or absence of sexual fantasies and desire for sexual activity" which causes the person distress or problems with other people, and which is not due to some other problem, such as a medical condition or substance use. Basically, a person with this problem avoids any kind of sexual relationship, even with a spouse. This, of course, is hard on the relationship! It should be kept in mind, though, that sexual desire varies enormously among human beings. While not liking sex is certainly statistically abnormal, it is not necessarily psychologically abnormal.
This business of "causing distress" and "not due to other problems" is something you find in most of the descriptions of sexual disorders (and, in fact, of mental illnesses in general), so I won't repeat it. In the judgment of most people in the psychology business, if it doesn't bother you and it doesn't bother the people around you, it isn't likely to be a problem. But, if it has some other, more physical, basis, it should be dealt with under a separate heading.
A similar problem is called sexual aversion disorder. A person with this problem has considerable anxiety, fear, or disgust feelings regarding genital contact, either in general or to specific aspects of sex such as smells or secretions. Both the preceding problems are found more often in people who grew up in homes where sex was considered evil or dirty.
Female sexual arousal disorder is the inability to become excited, especially as evidenced by adequate physical responses such as lubrication. About 19% of women suffer from this disorder, so it is not rare! Of course, in the 1800's, this was actually expected of a woman.
The male version of this is called male erectile disorder, the inability to attain and maintain an adequate erection. About 10% of men have this problem. It is much more common among older men.
Then there are three problems involving orgasm. About 24% of women have female orgasmic disorder, which involves a long delay or absence of orgasm after normal sexual excitement. As you can see from the percentage, this can hardly be called an abnormality. It is really just the lower end of the normal distribution! The male parallel is called male orgasmic disorder, and it is a problem for about 8% of men.
Far more common is premature ejaculation, which is a matter of ejaculating after only a minimal amount of sexual stimulation. This is very common among young boys, especially in their first sexual experiences. Unfortunately, about 29% of men suffer from it, making it too just the lower end of the normal distribution. Interestingly, there have been many cultures that consider it perfectly normal to have an orgasm shortly upon penetration. In Ireland in the 1800's, some people considered it the proper thing to do, so as not to make the wife suffer from the indignities of sex too long!
Pain during sex is, of course, unfortunate whatever your culture. Dyspareunia is genital pain associated with intercourse. Although it can be felt by both men and women, it is far more common among women, 14% of whom suffer from it.
A particularly painful problem is called vaginismus. While contractions of the vagina are a normal part of sex, some women suffer from intensely painful contractions that prevent them from enjoying sexuality at all. Fortunately, it is rare.
Most of the preceding problems may also have other causes. Among the medical conditions that can cause sexual dysfunction are MS (multiple sclerosis), diabetes, disorders of the thyroid, adrenal glands, and the pituitary, heart and blood pressure problems, genital infections, and post-surgical complications. Many recreational drugs cause sexual problems, including alcohol, amphetamines, cocaine, opioids, sedatives, etc. Among the prescription drugs that have negative sexual side effects are anti-anxiety drugs, anti-depressants, blood pressure medication, epilepsy drugs, and steroids.
Paraphilias
A paraphilia (from the Greek, "beyond love") is a disorder that involves desires and behaviors associated with unusual stimuli. Psychologists again are not interested in people who simply have fantasies about such things - not unless they act on them and bother other people or are themselves disturbed by them.
The first group of paraphilias are ones that bother others (including the law!) more than the person who has the problem:
Exhibitionism is when a person likes to expose their genitalia, breasts, or buttocks to strangers. The usual term for these people is "flasher." It is mostly men, but there are a considerable number of women as well.
Voyeurism (from the
French word for
"watcher") is a matter of secretly observing others undressing or
engaging in sexual
acts. In common parlance, these people (usually men) are called
"peeping
Toms."

Antique pornography
Frotteurism (from the French word for "one who rubs") involves touching and rubbing against other people in the street, on crowded buses or trains, and so on. Again, it is mostly men, although in Japan, for example, it is as common among women as well.
In all three of these cases, the perpetrator becomes aroused and usually goes off to masturbate. You can see how these shade off into behaviors that are not considered pathological: It is not considered voyeurism, for example, when you watch a stripper or pornography. Neither is it considered exhibitionism if you take off your clothes or engage in sex for the viewing pleasure of others on a professional basis.
Perhaps the most common paraphilia is called fetishism (from Portuguese fetico, meaning "charmed"), a term coined by the inventor of the IQ test, Alfred Binet. Fetishism is a matter of getting aroused by certain objects, most commonly articles of clothing such as underwear, stockings, shoes, etc. There are many pretty unusual fetishes as well, which I shall leave to your imagination.
There is also something called transvestic fetishism, which is dressing in the clothes of the opposite sex for sexual stimulation. (This is not the same as transvestism associated with gender identity disorders, below.)
Fetishism is probably mostly learned by associating the object with sexual pleasure, especially during masturbation. As one might expect, fetishism is found more in men and usually starts in early teenage years.
More Dramatic Disorders
The terms sadism and masochism were coined by Krafft-Ebing: Sadism is named for the Marquis de Sade (1774-1814) writer of sadistic novels, and practitioner of same; Masochism is named for Leopold von Sacher-Masoch, who wrote novels involving the pleasures of pain. As you probably know, sadists find sexual arousal and satisfaction in hurting and humiliating others, while masochists find their pleasure in being hurt and humiliated.
The range of sado-masochism is huge: Many people enjoy occasional light spanking or biting. Some people play "games" involving bondage (tying someone up) and discipline (whipping or paddling) - usually involving a secret word that signals to the other that you want to stop. Rarer are people who enjoy peeing on someone or being peed on. A few people can only gain sexual satisfaction by actually being beaten, cut, pierced, or whipped, or doing so to another person, especially someone who is unwilling.
According to one study, 14% of men and 11% of women have had some sexual experience with sadomasochism (Janus & Janus, 1993). Another suggests that 5-10% of the U.S. engages in sadomasochism on at least an occasional basis, and that 11% of men and 17% of women have tried bondage (Lowe, Walter, The Playboy Readers' Sex Survey, 1983 - perhaps not the most reliable source!). Although many people believe that sado-masochism is a matter of personal decisions between consenting adults, I am concerned that mixing aggression or self-loathing with what should be a loving act sets a pretty dangerous precedent.
The most dangerous form of sado-masochism is something called hypoxyphilia. Usually, one person cuts off another's breathing with their hands, rope, or article of clothing during sex, in an effort to cause asphyxiation at the moment of orgasm. Presumably, this intensifies the orgasm considerably. This is also sometime done by the person him- or herself during sex or masturbation. Needless to say, occasionally people die.
Bestiality is having sexual relations with animals. It isn't quite as rare as one might think: Kinsey found that 17% of farm boys admitted to sex with animals. More recent research suggests that it is found primarily in young boys who are mentally deficient. However, interest in bestiality is making a comeback in the form of porn websites devoted to the practice.
The most hated sexual disorder is pedophilia or sexual activity with children. This is primarily an activity engaged in by men (although there are some women as well), and most of these people seem to lack adult sexual experience and to have strong feelings of inferiority and inadequacy. Preying on children apparently makes them feel powerful. Contrary to popular imagination, pedophilia is found more often among heterosexuals than homosexuals.
I don't really want to come across as making excuses for this behavior, but... there is a degree to which cultural variation has to be taken into account. There have been some cultures in the past (and a few in the present) where sexuality with adolescent and late prepubescent boys and girls was considered quite acceptable. There are also a number of cultures where stroking a young child's genitals is a way of calming the child! Where the culture supports it, there isn't the kind of psychological damage we usually associate with childhood sex.
Quite rightly, I believe, modern cultures see sex with preadolescent children as wrong, and even sex between teenagers and adults as a dangerous misuse of experience and power. The law may sometimes appear arbitrary in making judgments as to who is and who isn't a consenting adult, but that is unavoidable.
Some people are unhappy being whatever sex they are biologically or assigned by their culture or society. They feel that they were somehow put into the wrong body and want to be the other sex. This is called gender identity disorder.
It often involves transvestism - dressing in clothing of opposite sex. Sometimes, though, the person wants to go further and physically change their gender through hormone treatments and surgery. This is called transsexualism.
The hormone treatments cause the man to grow breasts and his beard to stop growing, or cause a woman to begin growing facial hair and develop a deeper voice. The surgery involved has become quite sophisticated, and they do a decent job in creating a realistic penis for women, or turning an unwanted penis into a fairly functional clitoris and vagina. This, of course, is not done without extensive psychological evaluation: The procedure is not reversible, after all!
One interesting note: Transsexualism is not tied to homosexuality. There are men who become women but still are attracted to women, and women who become men but are still attracted to men. Statistics on transsexualism are not available for the U.S. In Europe, however, one out of every 30,000 men and one out of every 100,000 women undergo sex-change surgery.
I do need to add one more point (I am writing this addendum in 2019): Quite a few people, especially younger people, are rejecting the notion that they must identify as one sex or the other, or one gender or the other. They may appear to others as hermaphroditic (male and female simultaneously) or they may dress or act in different ways on different days. They may prefer not to be called he or she. They may have no strong sexual inclination, or they may like to have sex with anyone (not just "bisexual" even, but "pansexual"). The gap between sex as a biological characteristic and gender as a sociocultural construct has widened enormously. Unfortunately, this has led to some negative reactions, and some of what homosexuals have had to suffer in the last century, now is being replayed by those who lack compassion. Let's hope we can weather this storm as we have had to weather so many before!