Prenatal development
Dr. C. George Boeree
Prenatal development
Dr. C. George Boeree
We don't often discuss prenatal development in psychology courses, but I think that's really inexcusable. If anything, it is the most significant segment of our development! So I have included this short chapter, adapted in large part from The Medical Encyclopedia, U.S. National Library of Medicine, available online at http://www.nlm.nih.gov/medlineplus/ency/article/002398.htm. I know many of you have seen all this before in other classes, but it is well worth the review!
After sexual intercourse, sperm travels through the cervix and
uterus
and into the Fallopian tubes. Conception usually takes place in
the
outer
third of the Fallopian tube. A single sperm penetrates that egg
and a
joining
of the genetic information occurs. This resulting single cell is
called
a zygote.
sperm entering egg
The zygote spends the next few days traveling down the Fallopian tube and rapidly multiplying the number of cells through division. A mulberry-like mass, like a hollow rubber ball, 1/100 inch wide, results from the cell division. This ball of cells in the Fallopian tube is called a morula.
With additional cell division, the morula becomes a blastocyte, with an inner core and an outer shell of cells. The outer group of cells become the membranes that nourish and protect the inner group of cells, which becomes the fetus.
The blastocyte implants in the uterus between the 7th and 9th day
after
conception. At this point the endometrium (the lining of the
uterus)
has
grown and is ready to support a fetus. The blastocyte burrows into
the
endometrium where it receives nourishment. It is barely visible,
but
doubles
every 24 hours. The placenta and supporting infrastructure for
pregnancy
develop at this time as well. It is estimated that up to 55%
of
zygotes
never reach this phase of growth.
The Embryo
The embryonic stage begins on the 15th day after conception and continues until about the 8th week, or until the embryo is 1.2 inches in length. During this period the cells of the embryo are not only multiplying, but they are taking on specific functions. This process is called tissue differentiation. It is during this critical period of differentiation (most of the first trimester or three-month period) that the growing fetus is most susceptible to damage from external sources (teratogens) including viral infections such as rubella, x-rays and other radiation, and poor nutrition.
A child who has one developmental problem may have other problems that arose at the same time: Kidney problems and hearing problems, for example, are often found together because both kidneys and the inner ears develop at the same time.
In Week 3 we see the formation of the heart, the beginning development of the brain and spinal cord, and the beginning of the gastrointestinal tract.
Teratogens introduced during this period may cause severe problems such as the absence of one or more limbs or a heart that is outside of the chest cavity at birth.
Weeks 4 and 5 -1/4 inch long: Here we see the beginnings of the vertebra, the lower jaw, the larynx ("voice box"), and the rudiments of the ear and eye. The heart, which is still outside body, now beats at a regular rhythm. Although arm and leg "buds" are visible with hand and foot "pads," the embryo still has a tail and cannot be distinguished from pig, rabbit, elephant, or chick embryo by an untrained eye.
Teratogens may cause very serious problems involving the
esophagus,
vertebrae, eyes. The baby could be born with severe facial
clefts
or missing hands or feet.

Week 6 - 1/2 inch, 1/1000 of an ounce: In week 6, we see the formation of the nose, jaw, palate, lung buds. The fingers and toes form, but may still be webbed. The tail is receding, and the heart is almost fully developed.
Teratogens at this point may leave the baby with profound heart problems or a cleft lip.
Week 7 - 7/8 inch, 1/30 ounce (less than an aspirin): This week, the eyes move forward on the face, and the eyelids and tongue begin to form. All essential organs have begun to form.
Teratogens may cause heart and lung problems, a cleft palate, and ambiguous genitalia (not quite male or female).
Week 8 -1 inch, 1/15 ounce: The embryo now resembles a human being. The facial features continue to develop and the external ear appears. Also, we see the beginnings of external genitalia. By now, the circulation through the umbilical cord is well developed. The long bones begin to form and the muscles are able to contract.
Teratogens may still cause heart problems and stunting of the
fingers
and toes.
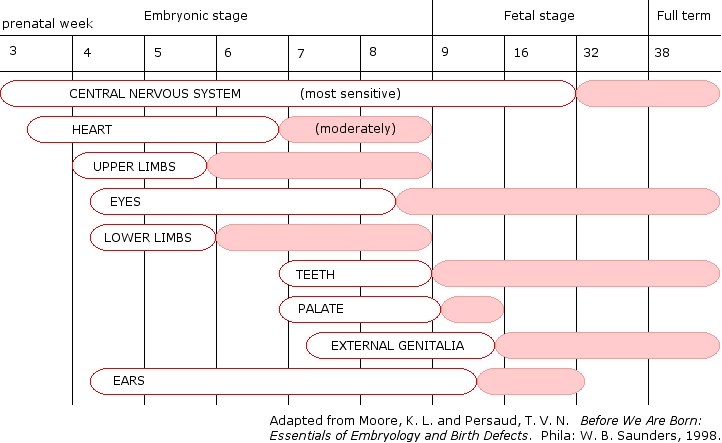
Timing of birth defects
The Fetus
At this point the embryo is developed enough to call a fetus. All organs and structures found in a full-term newborn are present.
Weeks 9 to 12 - 3 inches, 1 ounce: The head comprises
nearly
half of the fetus� size and the face is well formed. The
eyelids
close now and will not reopen until about the 28th week. The
tooth
buds for the baby teeth appear. The genitalia are now
clearly
male
or female.
Weeks 13 to 16 - 6 inches: These weeks mark the beginning of the second trimester. Although the skin of the fetus is almost transparent, fine hair develops on the head called lanugo. The fetus makes active movements, including sucking, which leads to some swallowing of the amniotic fluid. A thin dark substance called meconium is made in the intestinal tract. The heart beats120-150 beats per minute and brain waves detectable.
Weeks 17 to 20 - 8 inches: Eyebrows and lashes appear and nails appear on fingers and toes. This is an exciting time for the parents: The mother can feel the fetus moving ("quickening") and the fetal heartbeat can be heard with a stethoscope.
Weeks 21 to 24 - 11.2 inches, 1 lb. 10 oz.: All the eye components are developed, footprints and fingerprints are forming, and the entire body covered in cream-cheese-like vernix caseosa. The fetus now has a startle reflex.
Weeks 25 to 28 - 15 inches, 2 lbs. 11 oz.: Now we are entering the third trimester. During these weeks, we see rapid brain development. The nervous system is developed enough to control some body functions, and the eyelids open and close. A baby born at this time may survive, but the chances of complications and death are high.
Weeks 29 to 32 - 15 to 17 inches, 4 lbs. 6 oz.: These weeks see further development towards independent life: There is a rapid increase in the amount of body fat and the fetus begins storing its own iron, calcium, and phosphorus. The bones are fully developed, but still soft and pliable. There are rhythmic breathing movements present, the fetal body temperature is partially self-controlled, and there is increased central nervous system control over body functions.
Weeks 33 to 36 - 16 to 19 inches, 5 lbs. 12 oz. to 6 lbs. 12 oz.: The lanugo (body hair) begins to disappear. A baby born at 36 weeks has a high chance of survival.
Weeks 37 to 40 - 19 to 21 inches 7 or 8 pounds: At 38
weeks,
the fetus is considered full term. It fills the entire
uterus,
and
its head is the same size around as its shoulders. The
mother
supplies
the fetus with the antibodies it needs to protect it against
disease.
Birth
Birth has nearly as many dangers as the embryonic stage, mostly from infections and anoxia. Anoxia means "no oxygen," and can be due to a number of situations: If something prevents the exchange of blood from mother to child prior to the baby breathing on its own, the lack of oxygen quickly begins to take its toll, especially on the brain. This is called cord compression, and it can be caused by the cord being pressed between the baby's head and the mother's pelvis. A breech birth, which involves the baby's buttocks going first instead of its head, can slow the birth process. And premature separation of the placenta from the mother's uterus can cause anoxia as well.
Sometimes, it is necessary to perform a Caesarian section (or C-section) when such problems arise, in order to get the baby out more quickly. It is a fairly routine operation involving cutting the mother's abdomen and uterine wall. In emergencies, this is done with general anesthesia, but can also be done with spinal anesthesia, which allows the mother to remain awake and speeds her recovery time. It is, of course, still a serious surgical procedure and involves enough risks that a vaginal birth is usually preferred.
On a personal note: All three of my daughters were
delivered
by C-section, and my wife was awake for the second two. I
was
present
for those births, and the surgical nature of the deliveries did
not
detract
from our joy!

My grandson, Orion, soon after he was born
� Copyright 2003, 2009, C. George Boeree